
While surgery is appropriate for only a minority of people with back problems, approximately 45,000 Australians undergo spine surgery every year.
Continue readingWhile surgery is appropriate for only a minority of people with back problems, approximately 45,000 Australians undergo spine surgery every year.
Continue reading
All joint replacements in Australia since 2000 have been entered into a central registry run by the Australian Orthopaedic Association.
Continue reading
It was good to represent Ballarat as a Sports Physiotherapist at the National Basketball tournament being hosted here in Ballarat
Continue reading
Recently, The Age and Sydney Morning Herald carried headline articles on foot surgery being performed by podiatric “surgeons” without medical training. Channel Nine’s 60 Minutes programme also recently aired a story on this topic.
Continue reading
After a prolonged break due to the Covid 19 pandemic, we returned to Madagascar. Australian Doctors for Africa organise missions to provide medical services to the local people in Toliara, a town on the west coast of Madagascar, where services and infrastructure are lacking.
Continue readingIn the final training session before our first match, star Sam Kerr has injured her calf. We will all be hoping the team medical physicians and allied health practitioners can rehabilitate Sam quickly, particularly now as we have a critical must win game against Canada.
A strained calf muscle is a common injury in sports, and especially in ball sports. Proper rehabilitation following this type of injury is important to avoid re-injury. This blog focuses on the calf strain and how physicians working at Ballarat Sports Medicine can assist athletes with calf strains.
The muscles gastrocnemius and soleus, commonly referred to as the calf muscles, are located on the back of the lower leg. These muscles are particularly vulnerable to strains injuries. In football, they usually happen when a player quickly tries to reach the ball.
The middle part of the gastrocnemius muscle is most often injured. The strain is often in the superficial part of the muscle, i.e. towards the skin, just below the knee. Strain injuries in the soleus muscle are also quite common.
Signs and symptoms
The athlete will feel an acute “stabbing” or “cutting” pain and local tenderness. In addition, there is often swelling and visible bruising. The pain may cause the althlete to limp.
Diagnosis
The diagnosis is made by a doctor or physiotherapist following a clinical examination. MRI or ultrasound are not always necessary, but can be helpful in confirming the diagnosis.
Treatment and rehabilitation
In the acute phase (right after the injury occurs) it is important to start treatment according to the RICE principle (Rest, Ice, Compression, Elevation). This will help to reduce pain, minimize swelling, and prevent further damage.
Pain relieving medication is rarely necessary, but paracetamol can be taken if it is very painful. Pain killers can be effective in the first few days, but anti-inflammatories (NSAIDs) such as Nurofen, Voltaren and Naprosyn should be avoided for the first 24 hours. The reason for this is that they can have a blood thinning effect that can increase the amount of bleeding, resulting in more pain. In the beginning it can be a good idea to take some weight off the leg by using crutches. Following this, it is important to increase weight-bearing gradually. This will speed up recovery.
Exercises with a low load should be introduced early in the rehabilitation process. This will strengthen the new muscle tissue. Strengthening exercises can usually be started after 7-10 days. They should be done in consultation with a physiotherapist. Some passive treatment techniques (e.g. massage) can be helpful, but it is nevertheless systematic training that will have the best effect and greatest impact on the final result.
Later on, in the rehabilitation process, it is important for athletes planning on returning to sport to train maximum strength and jumping ability.
Skilled physiotherapists can assist with sport-specific rehabilitation at this point. Luke Blunden, Peta Johnston and Simon Lewis are all highly experienced clinicians who can direct your return to sport.
Prognosis
It is very difficult to predict how long it takes for a strained calf muscle to heal completely. This is often affected by the extent of the injury.
A study on professional football players showed an average time away from sport to be 13 days. In about 90% of cases, the athlete is back in full training within 28 days. Recovery from the most severe injuries can take up to several months.
There is a high risk of re-injury following this injury, especially for those who haven’t been through a comprehensive rehabilitation program.
https://fittoplay.org/body-parts/lower-leg/strained-calf-muscle/?p=4750
Excellence in healthcare is frequently driven by developments in research. This is no different in the fields of orthopaedic surgery and Sport & Exercise Medicine. Recently Mr David Mitchell and Mr Luke Spencer were co-authors of an article titled “Australian orthopaedic surgeons’ knowledge and practice of medial collateral ligament release in knee arthroscopy” published in ANZ Journal of Surgery. Additionally, Mr David Mitchell, Dr Greg Harris and Mr Like Spencer co-authored an article titled “The use of intra-articular platelet rich plasma for the symptomatic management of osteoarthritis of the knee: a pilot study” also published in ANZ Journal of Surgery. You can read this research at
https://onlinelibrary.wiley.com/doi/10.1111/ans.18001
https://onlinelibrary.wiley.com/doi/10.1111/ans.17565
The FIFA Women’s World Cup is under way. Australia have had success in the first game versus Ireland 1:0 albeit with the unfortunate loss of captain Sam Kerr to injury.
The injury that many sports persons dread and is relatively common in many sports is a rupture to the anterior cruciate ligament (ACL). This blog focuses on the ACL and how physicians working at Ballarat Sports Medicine and BallaratOSM can assist athletes with ACL injuries.
ACL Injuries
Anterior cruciate ligament (ACL) injuries are unpredictable. Most of them happen in harmless situations the athlete has been in hundreds of times before without it resulting in injury.
What many people do not know is, that we have two cruciate ligaments: An anterior and a posterior. Both are essential for stabilizing the knee. The anterior cruciate ligament is the one we hear most about. Unfortunately, usually after an injury has occurred.
This type of injury leads to a lengthy time away from sport (often up to 12 months) and increases the risk of osteoarthritis. Therefore, it is important that prevention of this type injury is a priority and if it does occur, that the right treatment is followed.
The knee’s safety belt
The ACL is a ligament in the centre of the knee that functions as a safety belt to prevent unwanted movements. A tear in the ACL is far more common than in the posterior cruciate ligament (PCL) and injuries to the former usually have a greater impact on knee function.
ACL injuries are especially common in sports that involve sudden changes in direction such as soccer. Female athletes have up to 3 times higher risk of an ACL injury than men and they are often injured at a young age.
Characteristics of a torn cruciate ligament
A typical characteristic of a cruciate ligament injury is swelling, which occurs soon after a twisting movement, and a sensation of giving way. It can also be difficult to straighten out the leg or bend the knee more than 80 to 90 degrees. You should have a medical examination if you show any of these signs. This can be arranged quickly with Sport & Exercise Medicine physician, Dr Greg Harris, or Sport & Exercise Medicine Registrar, Dr Jai Sharma at Ballarat Sports Medicine.
Additional injuries
Often, other structures such as the meniscus, cartilage, bone, and collateral ligaments, are also affected following a cruciate ligament injury. These additional injuries can often account for many of the symptoms following a torn cruciate ligament, and they can affect treatment options and the long-term prognosis. As such, it is important to have an MRI examination and get a specialist’s opinion soon after the incident.
Treatment
Surgery following an ACL injury is not a given. On the contrary, about 50% of ACL injuries are treated conservatively (rehabilitation without surgery). Many of these show good results.
An orthopaedic surgeon will evaluate whether or not knee surgery is required following an ACL injury. The decision is based on symptoms and the athlete’s requirements for knee function in the future. That means that surgery is more common for an elite soccer player. Independent surgeons, Mr David Mitchell and Mr Luke Spencer have subspeciality interest in knee injuries and can be seen quickly at BallaratOSM for ACL injuries.
It is recommended that athletes who don’t have any serious additional injuries try intensive training in conjunction with a physiotherapist for up to 3 months before surgery is considered. This will make it easier to predict whether the operation will have a good outcome, and rehabilitation will be more efficient. Luke Blunden, Peta Johnston and Simon Lewis are all highly skilled at assisting athletes at Ballarat Sports Medicine pre-operatively and post operatively with ACL injuries.
Surgery
The surgery involves replacing the injured ligament with tissue graft taken from the anterior or posterior thigh muscles. The surgery is done with an arthroscope using small incisions, which means that it is not necessary for the surgeon to completely open the knee.
Rehabilitation
Rehabilitation with a physiotherapist is tough following an ACL injury whether or not surgery is involved. Close monitoring of the training program is, therefore, important to manage all aspects of rehabilitation and a follow-up period of at least 6 to 12 months is recommended.
Rehabilitation focuses on regaining strength, mobility, balance, and control. The exercises are gradually made more difficult, and as function improves, more geared towards a functional return to the athlete’s sport.
For each extra month of post-surgery rehabilitation, the risk of re-injury is reduced by 50%. The athlete should pass a variety of sport-specific tests to check whether their knee is ready for returning to sport. But this in itself is not enough; the athlete should also feel that they are ready. It is important that the athlete is not overly worried about re-injury and that they can trust their knee.
The decision to return to sport should be made in consultation with the doctor, physiotherapist, trainer, and the athlete. Often, it is the trainer who knows the athlete best and sees how they move and behave in a sport-specific setting. Participation should also start slowly and be increased gradually.
Athletes with cruciate ligaments injuries have an increased risk of sustaining a new cruciate ligament injury, both in their injured and their uninjured knee. Ongoing preventative training is therefore especially important for this group.
Return to sport
Even though there are examples of elite athletes returning to competitive sport in less than 6 months, such an aggressive rehabilitation training program is not recommended. The risk of another injury to the knee is increased after a cruciate ligament injury but can be reduced by taking the time for proper rehabilitation.
References: https://fittoplay.org/sports/football/
A summary on meniscal injuries by Professor Romain Seal consultant knee and cartilage surgeon to Aspetar Sports and Orthopedic center of excellence can be viewed here
The FIFA Women’s World Cup is just days away. There are 8 groups of 4 teams in the first round robin stage. Australia will play Canada, Ireland and Nigeria after which the top two teams in our group will progress through to the knockout round of 16 matches.
After the FIFA Men’s World Cup, this will be the most watched sporting tournament world- wide. And Australia is hosting!!
This blog is the fourth in a series brought to you throughout the tournament where Ballarat Sports Medicine and BallaratOSM will focus on injuries in soccer. In this blog, the focus moves to the knee for Meniscal Injuries.
Meniscal Injuries
Meniscal injuries are among the most common knee injuries, and they come in different degrees of severity.
There are two different menisci in both knees. They lie on each side of the knee joint and function as shock absorbers and stabilisers. The meniscus on the inside is called the medial meniscus and the one on the outer part is called the lateral meniscus.
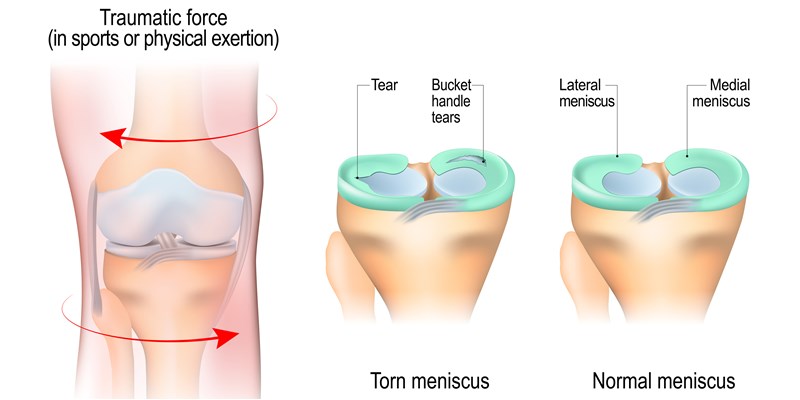
Twisting injuries
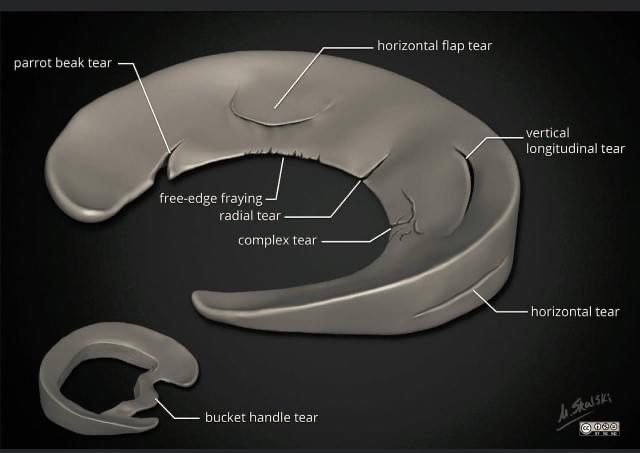
Meniscal injuries come in different forms which require different treatment approaches. Acute injuries occur when twisting the knee, and are most common in young athletes. Age-related changes or “injuries” in the menisci occur over time, affecting the middle-aged and the elderly. These age-related changes are a result of the body ageing on the inside, similar to what it does on the outside. Some hurt and some do not. Many knees have so called degenerative injuries (age-related changes), but no pain. We do not know exactly why that is.
Acute injuries often require surgery, either by removing part of the meniscus or by repairing it. The latter takes a long time to recover. Age-related changes are predominantly treated with a structured rehabilitation program and most recover without surgery.
Meniscal injuries can increase your risk of osteoarthritis. How big that risk is depends on the severity and location of the injury.
Injury mechanism, signs and symptoms
Most acute injuries are twisting injuries with the foot firmly placed on the ground. The degree of pain varies a lot. Some feel like something has been torn. Smaller injuries will not necessarily give immediate symptoms, but normally you will get pain and swelling within 24 hours after the injury occurred. With older athletes, a small tear in the meniscus can occur with minimal trauma.
Severe injuries normally give severe symptoms. Shortly after injury there is pain and decreased ability to bend and stretch the knee. It is also common the injured athlete can experience locking of the knee with or without clicking noises. This is also a common feature of anterior cruciate ligament (ACL) injury.
MRI imaging can help to determine the location and severity, but this is not always necessary.
Treating acute meniscus injuries
Treatment is dependent on the severity of the injury, size of tear, symptoms, and future requirements of the knee. On one end of the spectrum is a small tear, but without locking and limited range of motion. These might heal conservatively (without surgery) but sometimes follow-up shows they have not.
On the other end of the spectrum is severe and painful injuries, where the knee is locked in certain positions. These require immediate surgery with so-called arthroscopic surgery. This is keyhole surgery, using instruments that can be introduced through small (roughly 8-10mm) incisions. The decision to undergo surgery should be based on the severity of signs and symptoms, as well as the requirements for activity in the future.
Rehabilitation after surgery
Rehabilitation is affected by the severity of the injury. If a small piece of the meniscus has been removed, the athlete will be able to return to sport relatively quickly. Often within four weeks. More severe injuries with additional injuries to cartilage and ligaments will prolong the rehabilitation period. If the athlete returns to sport too early, it can have dire consequences. Recurrent swelling and persisting pain is often a result of this.
Rehabilitation should be done in conjunction with a skilled physiotherapist. The meniscus will gradually be able to withstand more weight-bearing activities. This should be incorporated in the rehabilitation program by gradually increasing physical requirements – if the knee can tolerate it.
Treatment of age-related injuries
Not so long ago, all meniscal injuries were treated the same – with surgery. Recent research, however, has shown that degenerative meniscal injuries should be treated with structured training. Exercises aim to strengthen the muscles around the knee, to increase body control and balance. It may take several months before the knee pain goes away, but results are as good as surgery.
Have a sore knee?
You can have your knee pain expertly diagnosed at Ballarat Sports Medicine. Sport & Exercise Medicine Physician, Dr Greg Harris and Sport & Exercise Medicine Registrar, Dr Jai Sharma can determine whether you may need surgery or not. If you do require surgery they may refer you to BallaratOSM’s independent surgeons, Mr Luke Spencer, Mr Shaun English, Mr David Mitchell, Mr Lawrence Tee, Mr Scott Mason or Mr Naveen Nara to assess the injury further with a view to provide surgical intervention to repair the damaged meniscus. Physiotherapists, Luke Blunden, Peta Johnston and Simon Lewis are all highly qualified to rehabilitate your knee.
References: https://fittoplay.org/sports/football/

Luke Blunden
APA Sports and Exercise Physiotherapist
Strength and Conditioning Coach
Australia’s FIFA Women’s World Cup team has been selected. A squad of 23, ranging in age from 21 (Kyra Cooney-Cross) to 38 (Aivi Luik). Our named captain is arguably the worlds best player, Sam Kerr and our vice-captain is Steph Catley. Our least experienced international representative is Clare Hunt having played just 5 matches for Australia, and our most capped player is Clare Polkinghorne with 156 matches. Only three of our players are currently playing for local teams, with the other 20 playing for teams from England, Sweden, USA, Norway and France. A great mix of talent and experience that we hope to see progress far into the tournament. But any player can suffer soft tissue injuries. Our independent practitioners will be watching the tournament intently, hoping all Australians remain injury free. They are all trained to treat elite athletes from any sport and plan their recovery and return to sport. The complimentary specialties that they offer, including Physiotherapy, Sport & Exercise Medicine, Exercise Physiology, Psychology and Myotherapy as well as immediate access to orthopaedic surgeons and practice nurses, provide all levels of athletes with healthcare options best suited to their needs.
This blog is the third in a series brought to you throughout the tournament where Ballarat Sports Medicine and BallaratOSM will focus on common injuries in soccer. In this blog we focus on Hamstring muscle injury
Hamstring injuries are one of the most common injuries in football. A hamstring injury is a strain or tear to the group of muscles at the back or posterior aspect of the thigh that occurs when one or more of the three muscles are strained or pulled beyond their capacity. Sports Medicine Physician Dr Ian Beasley from the Aspetar Sports and Orthopaedic centre of excellence provides a good overview here.
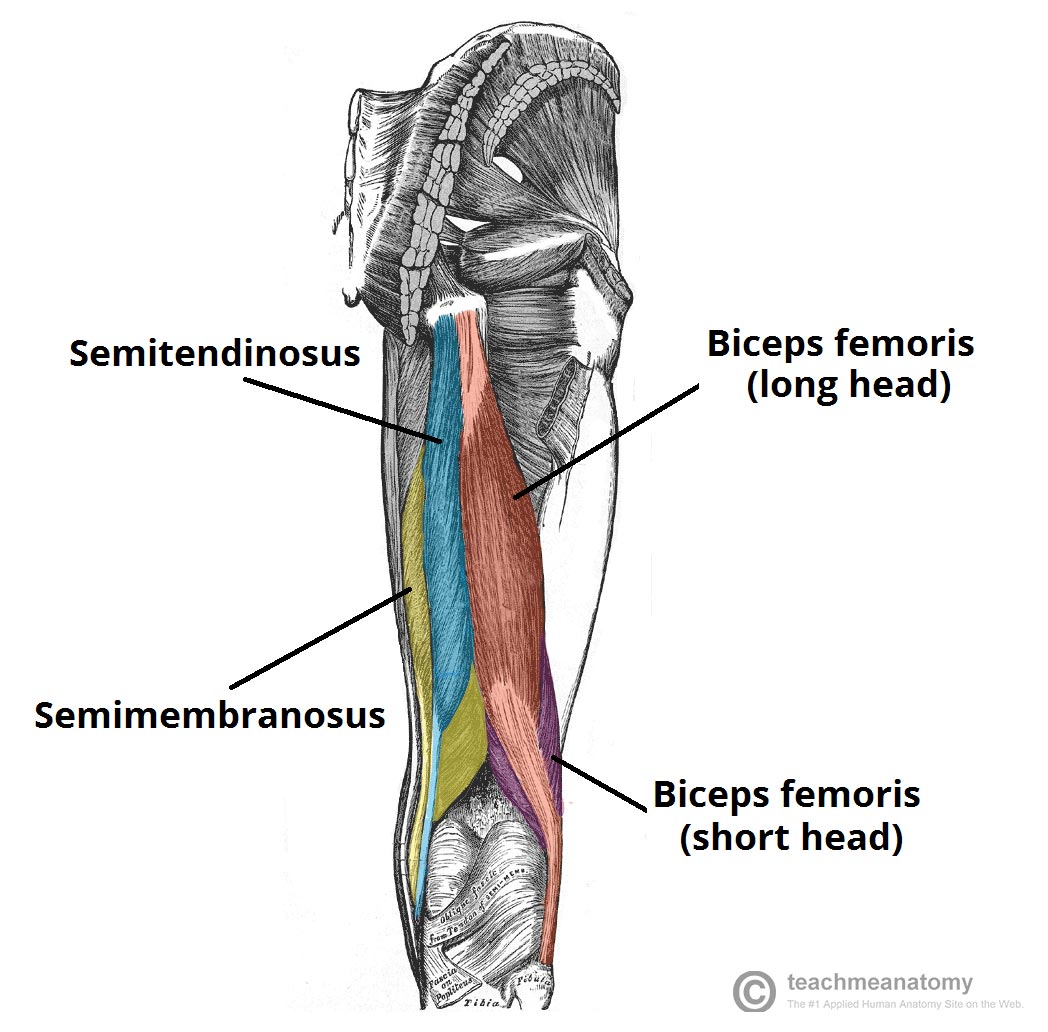
Anatomy
The three hamstring muscles are biceps femoris, semitendinosis and semi membrenosis. Each of these three muscles act together in their function however have differing anatomical function to allow the body to perform different elements of sporting performance. The attachments sites, muscle and tendon structure of the muscles differ and are specifically designed for a particular function and work in conjunction with other systems in the body. The hamstring muscle which crosses the knee and hip joint in basic terms acts to flex (bend) the knee and extend the hip when contracted in a shortening (concentric) action, however in a more dynamic context it also is involved in knee extension, hip flexion, rotation of the thigh and stability. A comprehensive understanding in how the hamstring muscle works is important in maximising recovery and performance.
Injury Grading
Hamstring muscles injury can be graded according to their severity;
The severity of injury will determine the degree of healing and recovery time required.
Signs and symptoms
Causes
Injury is typically caused from direct (contusion) or indirect (strain or distension) mechanisms. A contusion injury usually occurs from a direct blow from an opponent causing a ‘corkie’ where the opponent compresses the muscle between them and the players thigh bone.
A strain or tear is when the demands of the task the athlete is performing exceeds the capacity of the muscle unit.
Hamstring injury is associated with sports that involve;
Re injury of the hamstring muscle is common and can be a vicious cycle for athletes effected in terms of pain and dysfunction, reduced performance and time lost from sports.
Risk factors
Diagnosis
Diagnosis of hamstring injury begins with a clear history from the player, then a thorough physical examination that includes careful examination of range of motion and muscle contraction.
X-ray images can check for an associated avulsion fracture, while an ultrasound or MRI can visualise injury in the muscles or tendon. An MRI scan is a useful tool to determine the exact location and extent of injury.
Treatment
Most hamstring muscle injuries will be treated by a Physiotherapist with only a small amount requiring surgical intervention.
The initial goals of treatment will be;
Reduce pain and swelling
Restore mobility and walking
Restore flexibility and muscle strength
Restore function and performance
Surgery is required if the muscle is pulled away from its origin or insertion at the pelvis or shin bone or in some severe cases of tear to the muscle fibres. At Ballarat OSM we have a clear protocol for post operative management after hamstring surgery to return athletes to sport.
Return to sport
Our Physiotherapists in conjunction with the sports medicine team, athlete, coach, and parent will facilitate return to sport.
Common criteria for return to sport may include;
Prevention
Injury prevention is more desirable than muscle injury however is not usually given enough focus in community sport. Sports medicine teams will consider the injury profile of the sport and individual athletes when developing programs. For hamstring injuries prevention begins with considering the risk factors to injury and working on the modifiable risk factors.
Specific hamstring strengthening and sprinting are two well discussed areas for focus.
Some hamstring injury prevention programs that have been successfully implemented in elite and community sport can be found here and include Footy first, the netball knee program, FIFA 11+, and Prep to Play.
Ballarat Sports Medicine has elite Sports and Exercise Medicine Physicians, APA Sports and Exercise Physiotherapy and Advanced Exercise Physiology clinicians who can assist you with prevention or management of hamstring injury in life or sport.