Patella instability is rarely straightforward!
A presentation with a first time dislocation may look for a quick solution, but one needs to be wary when it isn’t going to work. The presence of patella alta, trochlear dysplasia, knock knees, rotational profile abnormalities and open growth plates all influence which of the surgical options are appropriate. We do know that splinting in an extension splint adds to quadriceps weakness, so at the very minimum, early physiotherapy and commence ROM exercises is appropriate. We know the success of MPFL repair (not reconstruction) isn’t great – even when the injury seems to be a pure avulsion from the patella, it’s not infrequent that the ligament was stretched first.
Indications for a reconstruction of the medial patellofemoral ligament include an apparent isolated injury to the MPFL in the absence of any other problem, or open growth plates with a need to do surgery before skeletal maturity. Open growth plates don’t prevent the surgery from being performed, the graft can be wrapped around the adductor tendon on the adductor tubercle, or a bone tunnel can be placed adjacent to the growth plate to avoid injury. Given the growth plate averages 2.7mm from Schott’s point in girls and 4.6mm in boys, a soft tissue solution is safer when further growth is expected. The MPFL origin is just proximal to the physis.

Lateral releases are not used as an isolated procedure, but might be incorporated into the operation. It is important to recenter the patella in the trochlear groove, and if a lateral retinacular lengthening or release is required, so be it.

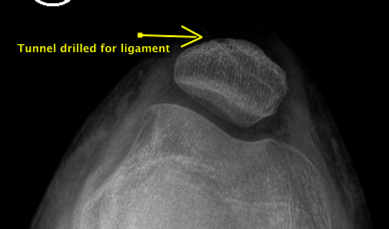
To get good integration between the ligament reconstruction and the patella, a tunnel through the cancellous bone improves results. The end of the reconstruction is then sewn to the retinaculum over the front of the patella, or woven into it in certain situations. To do all of this surgery a number of surgical incisions are required – but they generally fade well over time. The patients with underlying factors contributing to their patella dislocation might still need further surgery when the growth plates have closed.
Ref:Shea KS et al, The Relation of the femoral physics and the patellofemoral ligament. Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 26, No 8 (August), 2010: pp 1083-1087
Mr David Mitchell
Orthopaedic Surgeon
david.mitchell@ballaratosm.com.au
M 0438 322 969